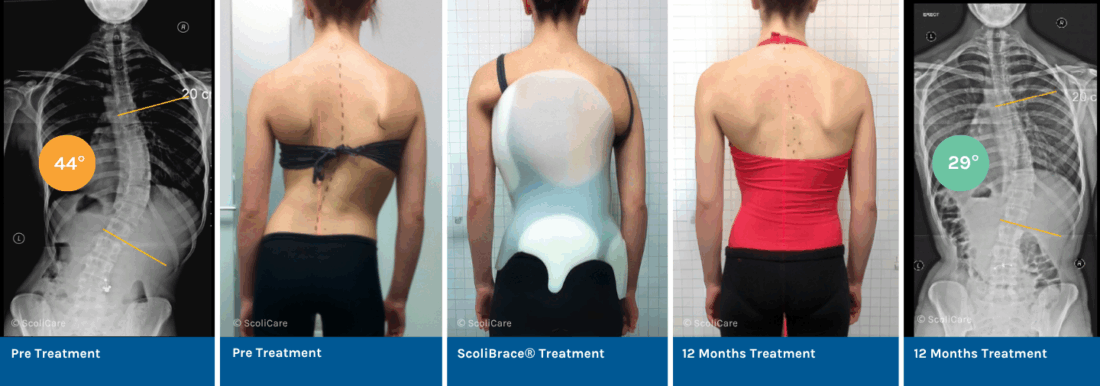
Reduction of a large thoracic scoliosis in a in a Ballet Dancer with ScoliBrace® and ScoliBalance®
At 17 years old, a young ballerina presented with a 44° thoracic Adolescent Idiopathic Scoliosis, postural asymmetry, and daily back pain (VAS 7–8/10). She was Risser 5, indicating she was skeletally mature. Hoping to avoid surgery and protect her flexibility for a future dance career, she pursued a non-surgical approach to treating her scoliosis.
She was prescribed a part-time ScoliBrace® (6–8 hrs/day) combined with the ScoliBalance® rehabilitation program performed twice daily at home. The goal was to improve posture, reduce pain, and prevent progression.
Results
- Curve Reduction: After 12 months, her thoracic scoliosis reduced from 44° to 29° (Cobb), a 15° (34%) reduction.
- Pain Relief: Pain levels dropped from daily moderate-severe to only occasional mild discomfort (VAS 2–3/10).
- Improved Posture & Function: Cosmetic asymmetry, rib humping, and scapular imbalance improved. She was also accepted into a prestigious overseas ballet program.
NB: Results vary from case to case. Our commitment is to recommend the most appropriate treatment based on the patients type and severity of scoliosis.
Looking for a non-surgical treatment approach for Adolescent Idiopathic Scoliosis? Connect with a ScoliBrace® provider near you to explore a custom bracing solution that fits your needs.