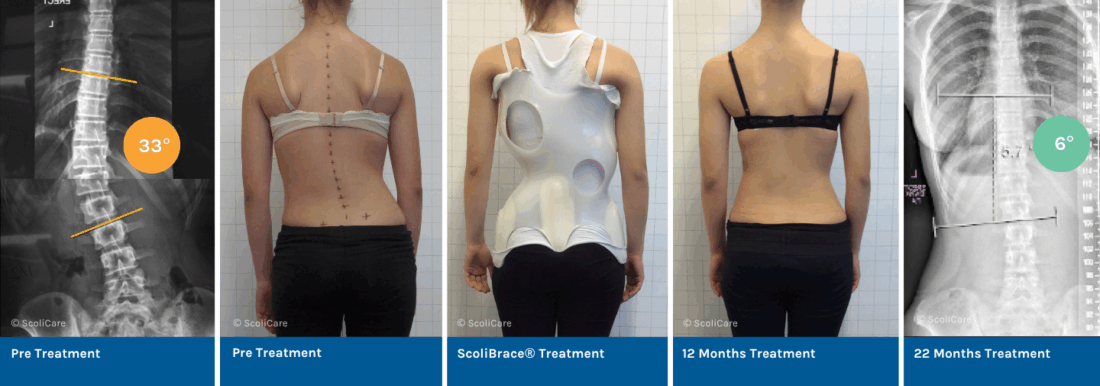
Correction of a 33° thoracolumbar Scoliosis using a ScoliBrace orthosis and Scoliosis Specific Rehabilitation
At age 13, the patient presented at the ScoliCare clinic following a diagnosis of adolescent idiopathic scoliosis (AIS). She was experiencing mild back pain and noticed asymmetry in her posture. Active in sports – ballet, dance, and netball – four times a week, her X-rays revealed a 33° left thoracolumbar scoliosis with a high risk of progression.
She was prescribed a full-time ScoliBrace® protocol combined with the ScoliBalance® rehabilitation program.
Results
- In-Brace Correction: One month after bracing, her scoliosis reduced significantly from 33° to 13° (61% reduction) on the in-brace X-ray.
- Long-Term Results: After completing treatment, out-of-brace X-rays showed a further reduction of the curve to 6°, a 27° (82%) Cobb angle reduction overall.
- Improved Function and Pain Relief: Her posture and pain greatly improved, and she is now pain-free, continuing her sports activities without discomfort.
NB: Results vary from case to case. Our commitment is to recommend the most appropriate treatment based on the patient’s individual case.
Interested in a non-surgical, proven approach to treating Adolescent Idiopathic Scoliosis? Get in touch with a ScoliBrace Provider near you to discuss your individual case and explore how custom bracing can make a difference.